




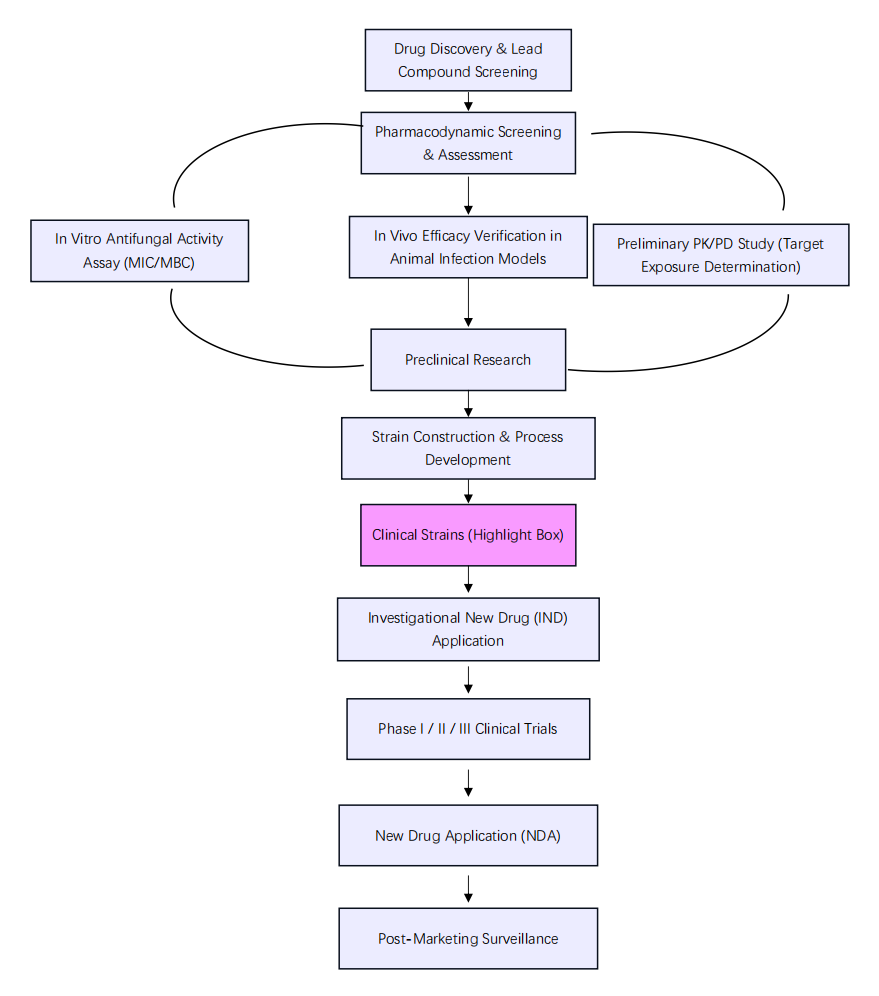
Figure 1. Flowchart of Antifungal Drug R&D and Registration Submission
Read On for Key Takeaways
Today we break down the core principles for selecting clinical isolates, packed with practical insights you won’t want to miss!
01 Regulatory Guidelines Set Clear Boundaries: Isolate Selection Is Not Arbitrary
Regulatory authorities including China’s NMPA, the U.S. FDA, and Europe’s EMA explicitly mandate that recent clinical isolates must be prioritized for in vitro pharmacodynamic studies (e.g., MIC measurement, time-kill curve assays) and in vivo model validation of antifungal agents, rather than over-passaged laboratory reference strains alone[2,3].

Root Cause
Only clinical isolates carry the actual resistance profiles and epidemiological trends prevalent in real-world clinical settings. Take Candida species as an example: data from the China Hospital Invasive Fungal Surveillance Net (CHINET) indicates that fluconazole resistance in Candida tropicalis neared 20% in certain years, while echinocandin resistance among Candida glabrata has risen year-on-year[4]. Even perfect efficacy data generated using reference strains isolated two decades ago may fail to translate to modern clinical practice. Regulators demand reproducible outcomes reflective of real patient treatment, not idealized laboratory activity.
02 Clinical Isolates: The Uncompromising Litmus Test for Authentic Drug Efficacy
Reference strains (e.g., ATCC strains) resemble docile laboratory animals. After decades of serial passaging, many virulence factors and resistance genes have been attenuated or lost, making them unable to recapitulate the true phenotypic traits of fungi causing clinical infections.
Case Illustration
A candidate antifungal agent yielded an impressive MIC value of merely 0.125 μg/mL against reference Candida albicans, yet its MIC surged to >16 μg/mL when tested against drug-resistant clinical isolates—this hundred-fold disparity is far from an isolated incident. Registration submissions relying solely on reference strain data inherently overestimate therapeutic potency, virtually dooming subsequent clinical trials to poor outcomes.03 Isolate Quantity and Diversity: The Minimum Threshold for Regulatory Review
Many pharmaceutical developers assume that simply incorporating clinical isolates satisfies regulatory requirements, yet reviewers assess not only presence but also sufficiency. Major regulatory bodies expect in vitro activity data covering dozens to hundreds of distinct clinical isolates for antifungal candidates[3,5]. This requires systematic evaluation not only of Candida albicans, but also non-albicans Candida species (C. glabrata, C. krusei, C. parapsilosis, C. tropicalis) and Aspergillus spp. (A. fumigatus, A. flavus, A. terreus, etc.). Novel antifungals additionally demand activity profiling against rare opportunistic fungi such as Mucorales and Fusarium—obtaining validated clinical isolates of these pathogens poses the greatest experimental hurdle.
Clinical isolates are primarily recovered from hospital clinical laboratories, yet their use entails strict oversight of patient privacy and biosafety. Full ethical approval and BSL-2 or higher-level pathogen laboratory registration are compulsory, resulting in lengthy, cumbersome workflows. Small biotech firms face prohibitive costs for in-house strain bank construction, while commercially sourced isolates often lack regional representativeness: isolates collected from European and American patients fail to mirror resistance patterns observed in Asian populations.
Mitigation Strategies
At present, only a handful of CROs in China operate large-scale, ethically compliant, commercially available clinical fungal strain repositories. We have established collaborative partnerships with numerous tertiary hospitals and regional anti-infective consortia to build a domestic pathogen resource platform covering major Chinese regions with complete ethical documentation chains.To address urgent project demands, we offer the following support:
·Assisted compliant procurement: We maintain established partnerships with qualified national and international culture collection centers, enabling clients to obtain ethically approved, fully identified clinical isolates without navigating complex regulatory workflows independently.
·Targeted hospital coordination: For clients requiring isolates from specific geographic regions or with defined resistance phenotypes, our hospital collaboration network facilitates targeted strain collection, paired with standardized ethical review and informed consent templates to cut communication and timeline costs.
·Strain identification and quality control services: Regardless of isolate sourcing channels, we deliver full identification and QC testing to ensure all raw data is traceable for regulatory inspection.
Challenge 2: Inaccurate Species Identification – Undermining the Entire Dataset Foundation
Fungi exhibit highly variable morphological characteristics, with countless morphovariants within the Aspergillus genus complicating visual discrimination. Conventional biochemical identification carries substantial misclassification risks. Misidentifying intrinsically fluconazole-resistant Candida krusei as Candida albicans, for instance, completely skews pharmacodynamic assessment. Even minor flaws in strain identification can prompt regulatory reviewers to question the scientific validity of an entire dataset.
Mitigation Strategy
We deploy the industry gold-standard dual identification workflow: MALDI-TOF mass spectrometry combined with Sanger sequencing of the ITS region and housekeeping genes (β-tubulin, calmodulin, etc.)[7,8]. Every client receives a full molecular identification report, raw sequencing electropherograms, and corresponding GenBank accession numbers to guarantee full traceability during regulatory audits.Challenge 3: Volatile Resistance Phenotypes – Compromising Experimental Reproducibility
Many clinical isolates are genetically unstable: Candida glabrata, for example, readily loses resistance plasmids upon serial passaging, leading to inconsistent MIC readings across three replicate tests. Regulatory guidelines mandate a minimum of three independent biological replicates per isolate, and unstable strains drastically extend experimental timelines.
Mitigation Strategy
All isolates are archived via ultra-low-temperature (-80°C) cryopreservation, with serial passages strictly capped at ≤3 generations post-banking. This preserves resistance profiles and virulence traits matching the original patient-derived isolate. We also supply strain stability validation data to pre-empt regulatory inquiries regarding experimental reproducibility.
KCI・KMQ Anti-Infective Vaccine & Drug R&D Service Platform
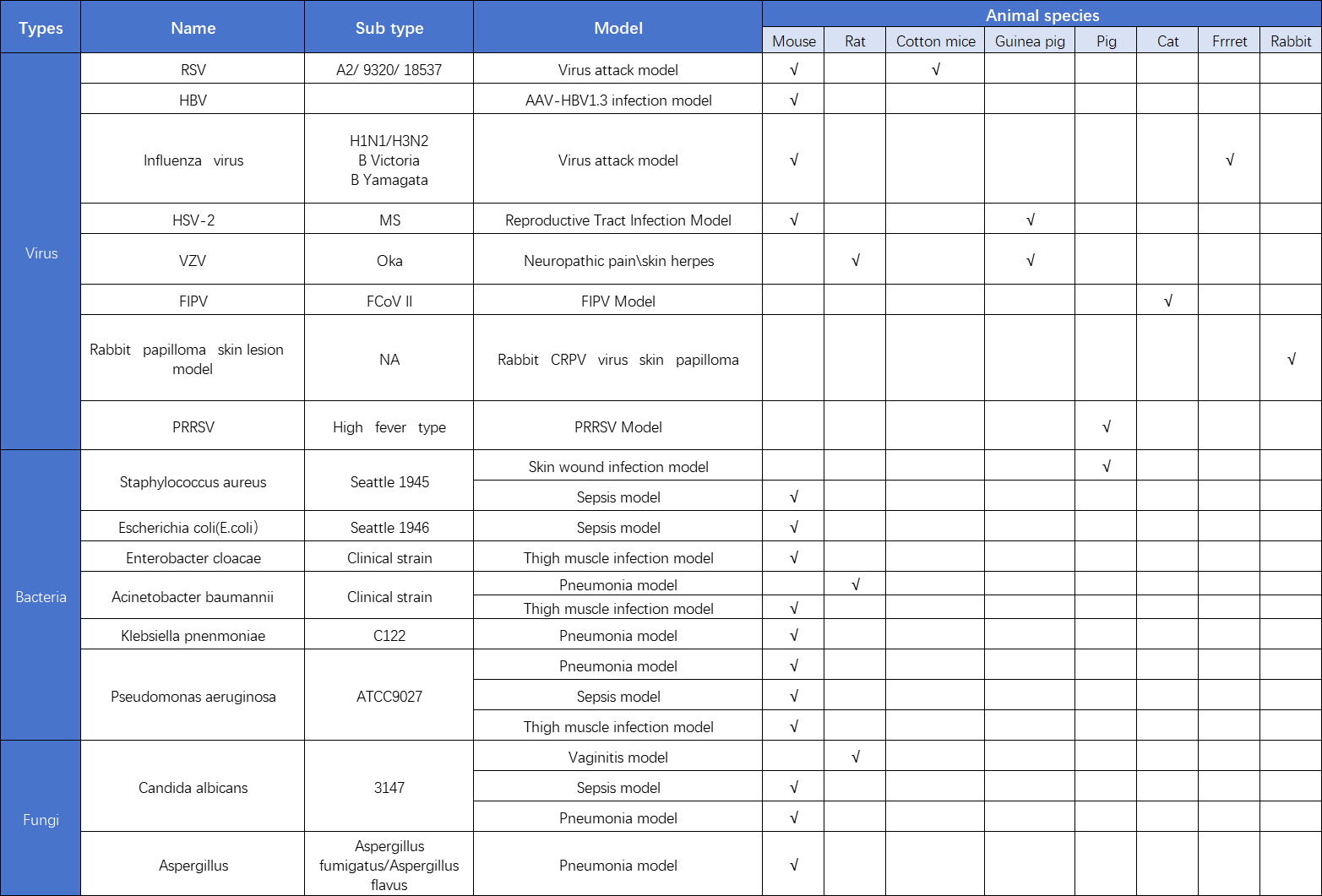
KCI・KMQ holds dual BSL-2 and ABSL-2 certifications and has built an integrated anti-infective R&D service platform covering more than 100 pathogenic microorganisms (bacteria, viruses and fungi) to support the development of human pharmaceuticals, veterinary drugs and pet medicines.The BSL-2 laboratory covers an area of approximately 200 m², with dedicated functional zones for cell culture, virology and bacteriology research. The ABSL-2 laboratory spans around 1000 m², consisting of a 300 m² small-animal testing wing and a 700 m² large-animal testing wing.
·In vitro anti-infective pharmacodynamic assays: Antiviral potency testing (EC₅₀/CC₅₀ quantification), MIC susceptibility testing, fractional inhibitory concentration (FIC) index measurement, assessment of impacts on pathogen biological characteristics, etc.
·In vivo vaccine immunogenicity assays: Neutralization tests, hemagglutination inhibition assays, cellular immunity evaluation, etc.
·In vivo pathogen challenge efficacy studies: For vaccines and antiviral agents
·General infectious animal model testing

·Is complete clinical medication history available for each isolate? (Isolates sourced from patients receiving fluconazole treatment are highly likely to carry induced drug resistance.)
·Is full traceability available for molecular identification records? (Are raw sequencing electropherograms and corresponding GenBank accession numbers complete and retrievable?)
·Which CLSI or EUCAST susceptibility breakpoints were adopted for MIC interpretation? For novel antifungals without standardized breakpoints, have MIC₅₀ and MIC₉₀ datasets been provided?
These inquiries directly determine whether your isolate data will gain regulatory acceptance or face critical scrutiny. Our team integrates comprehensive supporting documentation addressing all these points into study designs at the early stage, delivering a fully robust dossier that stands unassailable during regulatory review.
We fully recognize the immense challenges of building a large-scale, ethically compliant national repository of clinical fungal isolates in China. This undertaking requires long-term investment, cross-institutional trust, continuous communication with numerous hospitals, and rigorous progression of ethical approval paperwork. We invite all industry partners to advance this initiative together.
The obstacles surrounding clinical isolates are not individual burdens—they are shared challenges that we resolve collaboratively.
Let’s Have a Discussion
Which stage of your antifungal drug project is currently stalled? What types of isolates are you short of? Feel free to leave your comments below.
If you are a clinical laboratory professional from hospitals, we also welcome you to get in touch with us. We are seeking like-minded partners to collaborate on clinical isolate resources.

References:
1.Brown GD, Denning DW, Gow NA, et al. Hidden killers: human fungal infections. Science Translational Medicine. 2012;4(165):165rv13.
2.U.S. Food and Drug Administration. Antibacterial Therapies for Patients With an Unmet Medical Need for the Treatment of Serious Bacterial Diseases – Questions and Answers (Revision 1). 2017.
3.European Medicines Agency. Guideline on the evaluation of medicinal products indicated for treatment of bacterial infections. CPMP/EWP/558/95 rev 2. 2011.
4.China Hospital Invasive Fungal Surveillance Net (CHINET). Annual National Antimicrobial Resistance Surveillance Reports.
5.Clinical and Laboratory Standards Institute (CLSI). M27M44S: Performance Standards for Antifungal Susceptibility Testing of Yeasts. 3rd ed. 2022.
6.Ministry of Health of the People’s Republic of China. List of Pathogenic Microorganisms Transmissible to Humans. 2006.
7.Clinical and Laboratory Standards Institute (CLSI). M54: Principles and Procedures for Detection and Identification of Fungi in Clinical Specimens. 2nd ed. 2021.
8.Clinical and Laboratory Standards Institute (CLSI). M38: Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi. 3rd ed. 2017.
9.Lepak AJ, Andes DR. Antifungal pharmacokinetics and pharmacodynamics. Cold Spring Harbor Perspectives in Medicine. 2014;5(5):a019653.